 FP1130 : Efficacy of intralesional bleomycin in treatment of orbital lymphangiomas
FP1130 : Efficacy of intralesional bleomycin in treatment of orbital lymphangiomasDR. SINDHUJA MURUGESAN
Dr. VIJI RANGARAJAN
Semifinal
Abstract
Objective:To study the effectiveness of intralesional bleomycin injection in orbital lymphangiomas.
Methods: 16 patients diagnosed with orbital lymphangiomas were included in this prospective study. All of them received intralesional bleomycin injection at a dose of 0.5mg/kg body weight(maximum 15mg) along with 2% lignocaine. Patients who required repeat injections was based on the documentation of serial clinical and radiological response to treatment. Repeat injections were given once in every 4 weeks.
Results: Proptosis and lid swelling were the common presenting sign. All patients were treated with 2-4 injections of bleomycin. The follow up period ranged from 6-18 months. 11 patients had complete resolution, 3 patients had poor response and required surgical excision and remaining 2 patients had recurrence.
Conclusion: Intralesional bleomycin therapy is an effective and safe method of treatment of orbital lymphangioma without any significant ophthalmic or systemic side effects.
Full Text
Objective:
To study the effectiveness of intralesional bleomycin injection in orbital lymphangiomas. Methods: 16 patients diagnosed with orbital lymphangiomas were included in this prospective study. All of them received intralesional bleomycin injection at a dose of 0.5mg/kg body weight (maximum 15mg) along with 2% lignocaine. Patients who required repeat injections were based on the documentation of serial clinical and radiological response to treatment. Repeat injections were given once in every 4 weeks.
Results:
Proptosis and lid swelling was the common presenting sign. All patients were treated with 2-4 injections of bleomycin. The follow up period ranged from 6-18 months. 11 patients had complete resolution, 3 patients had poor response and required surgical excision and remaining 2 patients had recurrence. Conclusion: Intralesional bleomycin therapy is an effective and safe method of treatment of orbital lymphangioma without any significant ophthalmic or systemic side effects.
KEYWORDS:
ORBITAL LYMPHANGIOMA, BLEOMYCIN, PROPTOSIS
INTRODUCTION:
Lymphangiomas are benign lymphatic tumors, characterized by proliferation of anomalous dilated lymphatic vessels lined by normal endothelial cells.1, 2 Initially considered as a neoplasm, now the International Society for the Study of Vascular Anomalies (ISSVA) has classified lymphangiomas as combined vascular malformations within the spectrum of arterial, venous and lymphatic lesions that have characteristics of venous and lymphatic components.3, 4 Orbital lymphangioma represents 0.3%–4% of all orbital tumors.5 Depending on the location they can be classified as deep or superficial lymphangiomas.6 They can remain silent clinically or enlarge slowly causing proptosis, extraocular motility restriction and sudden engorgement due to intralesional haemorrhage causing compressive optic neuropathy.7 Ideally surgical excision is the main stay of treatment but due the extensive infiltrative nature of the lesion, complete surgical excision is dangerous due to risk of damage to adjacent vital structures. Hence recurrence is very common in case of incomplete removal of the lesion.8 Therefore, non-surgical methods such as intralesional sclerosing agents have been tried.2 In our study we have assessed the role and efficacy of intralesional bleomycin in orbital lymphangiomas in 16 patients.
METHODS:
This prospective interventional clinical study was conducted from September 2019 to September 2021. Sixteen patients with orbital lymphangiomas, diagnosed clinically and radiologically were included in this study. Patients who had hypersensitivity to bleomycin, impaired renal function test, pulmonary problems, pregnant or lactating women, and patients who lost to follow-up were excluded from this study. All 16 patients underwent detailed ophthalmological examination, including visual acuity, refraction, slit-lamp examination, applanation tonometry and fundus examination. Magnetic resonance imaging of the orbit was done for all patients. Systemic evaluation was also carried out along with routine blood investigations, ESR, renal and liver function tests. Serial photographs were taken and documented throughout the course of treatment and follow-up. Informed written consent was taken from all patients.
Bleomycin is commercially available in a dried powder form containing 15 international units (IU). 1 IU of bleomycin is equivalent to 1 mg of bleomycin. The dose for treatment of orbital lymphangiomas was estimated to be 0.5 IU/kg body weight and the maximum cumulative dose should not exceed 5 IU/kg body weight. Bleomycin solution was prepared with normal saline and 2% lignocaine at the ratio of 1:1. The volume injected into the lesion was proportional to the volume of the aspirate from the lesion (preferably 20% of the aspirate) but did not exceed 5 ml at a session.
The procedure was done under general anesthesia for children (<18 years of age) and with topical anesthesia along with sedation for adults. The reconstituted solution was injected intralesioally using a 23-gauge needle with 10cc syringe for aspiration. For deep intraconal lesions ultrasound guided injection was given. (Figure 1) First aspiration of the contents of the lymphangiomatous cysts was done and the fluid was sent for cytological testing. The needle was kept in the same position and bleomycin was injected keeping the total volume of the injected solution around 20% of that of the aspirate.
Injection of larger volume can cause extravasation of the drug, inadequate dispersion of the drug and compressive effects. Immediately after the procedure local pressure was applied to prevent leakage of bleomycin. Pupillary reactions and visual acuity were checked for a couple of hours following injection. Patients were reviewed on the first day postoperatively and again at 2 weeks. Those who required repeat injections were treated at intervals of 4 weeks. Treatment was discontinued after a maximum of 3 injections or when no further sign of resolution was noticed clinically. MRI scan of the orbit was repeated 6 months after the last injection to document the radiological evidence of resolution or any recurrence. Patients were under follow-up upto 1 year after completion of the treatment course.
RESULTS:
In our study out of the total 16 patients, 10 were females (62%) and 6 were males (38%). Five patients were in the paediatric group (< 16 years of age). All patients had unilateral presentation. Proptosis was the most common symptom (56%), followed by lid swelling (44%). Four patients with lid swelling had associated conjunctival mass as well. Two patients with proptosis had associated squint and ptosis. Table 1 summarizes the demographic and clinical profile of the patients.
The number of bleomycin injections ranged from 2 to 4, 8 patients (50%) had a complete resolution after 2 injections and 3 patients (19%) required 4 injections for satisfactory outcome. (Figure 2) Two patients (12%) after 3 injections resolution was noted but at follow-up at 6 months recurrence was noted. Rest three patients (19%) after giving the maximum cumulative dose no resolution was noted clinically or radiologically, hence debulking or complete surgical excision was performed. Table 2 summarizes the outcome and frequency of bleomycin injections in individual patients.
In our study immediate postoperative complications were pain at injection site, lid edema, ecchymosis and transient increase in proptosis. (Table 3 ) No long-term or systemic complications were noted.
DISCUSSION:
Lymphangiomas are benign hamartomatous lymphatic malformations most commonly seen in the head and neck region. They are thought to arise due to failure of the lymphatics to connect to the venous system, abnormal budding of lymphatic tissue, and sequestered lymphatic rests that retain their embryonic growth potential.1 These lymphatic rests can penetrate adjacent structures or dissect along fascial planes and eventually become canalized.1 These spaces retain their secretions and develop cystic components because of the lack of a venous outflow tract.
Radiologically lymphangiomas are characterized by multicystic lesions with
pathognomonic fluid levels.2 (Figure 3 )They may be isointense on T1-weighted MR imaging, but hyperintense on T2-weighted imaging with internal septations. Fat-suppressed images of the orbit are useful to highlight the presence of lymphangiomas against otherwise isointense fat. Contrast enhancement is not seen. Absence of flow voids and enlarged feeder vessels distinguish these lesions from high-flow lesions such as infantile hemangioma and arteriovenous malformations.2
Histologically, lymphangiomas are composed of dilated channels and multiple cysts lined with a single layer of endothelium. The stroma often contains lymphoid aggregates, macrophages, and fibrous septa.9
Orbital lymphangiomas are usually not recognized clinically at birth but becomes evident after episodes of upper respiratory tract infection, trauma, or sudden hemorrhage into the lesion.10 It often impose an increased risk for the development of painful proptosis, amblyopia, strabismus and compressive optic neuropathy. Ideally surgical excision is the main stay of treatment but due the extensive infiltrative nature of the lesion complete surgical excision is dangerous as there is risk of damage to adjacent vital structures 2 and incomplete excision can lead to recurrence.8 Sclerosants that have been used for orbital and extraorbital lymphangiomas include sodium morrhuate, sodium tetradecyl sulfate, ethanol, bleomycin, and doxycycline. 1 These agents can cause pressure effect in the orbit due to the volume of the injection and the edema.11
Bleomycin was first used as as antineoplastic antibiotic that was isolated from the fungus Streptomyces verticillus by Umezawa in 1966.12 Its acts by causing single- or double-strand DNA breaks and inhibition of DNA and RNA synthesis. 10 It is also causes induction of tumor necrosis factor and apoptosis in rapidly dividing cells.13 Its sclerosing effect on the vascular endothelium was first observed in the treatment of malignant pleural effusions. This led to its first use for treatment of lymphangiomas in 1977 by Yura and colleagues.14 The mechanism of action of bleomycin involves apoptosis of rapidly dividing cells and inhibition of DNA synthesis and involution of the lesion by fibrosis due to induced inflammation.2
The solution of bleomycin is prepared by addition of 2% lignocaine along with normal saline at the ratio of 1:1.The presence of lignocaine in the solution reduces discomfort for the patient postoperatively and also facilitates the dispersion of bleomycin into the cell by making the cellular membranes more permeable.7
There are no reports of major systemic adverse effects with the use of intralesional bleomycin in the orbit or elsewhere. Systemic side effects of bleomycin include fever, nausea, vomiting, injection site reactions, loss of appetite, weight loss, pulmonary toxicity (pneumonitis and pulmonary fibrosis), and injection site skin necrosis.13 We did not see any adverse reaction in any of our patients. Pulmonary fibrosis is dose dependent, and fatal pulmonary fibrosis occurs when cumulative dose exceeds 400 mg.1
Gooding and Meyer described bleomycin as a potential treatment for refractory orbital lymphangiomas, showing satisfactory outcome in 4cases.13 Kumar et al had a satisfactory response in 95% of non-orbital lymphangiomas treated with bleomycin.1 Raichura et al reported a dramatic response in 13 patients with orbital lymphangioma who were treated with intralesional bleomycin injection.2 Nuruddin et al also stated the effectiveness of intralesional bleomycin in orbital lymphangiomas.7
In our study, the common presenting symptom was proptosis and lid swelling. 8 patients had a complete resolution after 2 injections and 3 patients required 4 injections for satisfactory outcome. Two patients after 3 injections resolution were noted but at follow-up at 6 months recurrence was seen. Rest three patients after giving the maximum cumulative dose no resolution was noted clinically or radiologically, hence debulking or complete surgical excision was performed. In our study no systemic or serious local complications were noted.
CONCLUSION:
Intralesional bleomycin therapy is an effective and safe method of treatment of orbital lymphangioma without any significant ophthalmic or systemic side effects. It is a good alternative to surgical excision where it is not possible to remove the entire mass, and the patient is also concerned about cosmesis. It can also be used as an adjunct therapy to surgical debulking, where continuous negative pressure prevents chances of recurrence.
References
1. Kumar V, Kumar P, Pandey A, Gupta DK, Shukla RC, Sharma SP, et al. Intralesional bleomycin in lymphangioma: An effective and safe non-operative modality of treatment. J Cutan Aesthet Surg 2012;5:133-6.
2. Raichura ND, Alam S, Noronha VO, Mukherjee B, A prospective study of the role of intralesional bleomycin in orbital lymphangioma, Journal of AAPOS (2017), doi: 10.1016/j.jaapos.2017.03.007
3. International Society for the Study of VascularAnomalies [Internet]. Classification of Vascular Anomalies [cited 2016 April 18].
4. Nassiri N, Rootman J, Rootman DB, Goldberg RA. Orbital lymphaticovenous malformations: current and future treatments. Surv Ophthalmol 2015;60:383-405.
5. Russin JJ, Rangel‑Castilla L, Kalani YS, Spetzler RF. Surgical management, outcomes and recurrence rate of orbital lymphangiomas. JSM Neurosurg Spine 2014;2:1030.
6. Bansal S, Das S. Intralesional bleomycin: A treatment modality for conjunctival lymphangioma. Oman J Ophthalmol 2019;13:43-5.
7. Nuruddin M, Roy S, R, Singh Mudhar H: Results of Intralesional Bleomycin Sclerotherapy for Treatment of Orbital Lymphangiomas at a Tertiary Eye Care Centre in Bangladesh. Ocul Oncol Pathol 2019;5:412-417. doi: 10.1159/000495248
8. Stacey AW, Gemmete JJ, Kahana A. Management of orbital and periocular vascular anomalies.Ophthal Plast Reconstr Surg 2015;31:427-36.
9. Murat Tunç, Ehsan Sadri, Devron H Char. Orbital lymphangioma: an analysis of 26 patients. Br J Ophthalmol1999;83:76-80.
10. Rozman Z, Thambidorai RR, Zaleha AM, Zakaria Z, Zulfiqar MA. Lymphangioma: is intralesional bleomycin sclerotherapy effective?Biomed Imaging Interv J2011;7:e18.
11. Kalisa P, Van Zieleghem B, Roux P, Meire F. Orbital lymphangioma: clinical features and management. Bull Soc Belge Ophtalmol 2001;282:59-68.
12. Umezawa H. Recent study on biochemistry and action of Bleomycin. In: Carter SK, Crook ST, Umezawa H, editors. Bleomycin: Current Status and New Developments. New York (NY): Academic Press; 1978. pp. 15–20
13. Gooding C, Meyer D. Intralesional bleomycin: a potential treatment for refractory orbital lymphangiomas. Ophthal Plast Reconstr Surg2014;30:65-7.
14. Yura J, Hashimoto T, Tsuruga N, Shibata K. Bleomycintreatment for cystic hygroma in children. Arch Jpn Chir 1977;46:607-14.
Table 1 CLINICAL SUMMARY OF PATIENTS
| S.NO | AGE/SEX | LATERALITY | COMPLAINTS |
|---|---|---|---|
| 1 | 5 YEARS/MALE | RIGHT | LID SWELLING |
| 2 | 10 YEARS/FEMALE | RIGHT | PROPTOSIS |
| 3 | 10 YEARS/MALE | LEFT | LID SWELLING WITH CONJUNCTIVAL SWELLING |
| 4 | 8 YEARS/FEMALE | RIGHT | LID SWELLING |
| 5 | 5 YEARS/FEMALE | RIGHT | PROPTOSIS WITH SQUINT |
| 6 | 34 YEARS/MALE | LEFT | PROPTOSIS WITH SQUINT |
| 7 | 50 YEARS/FEMALE | LEFT | PROPTOSIS |
| 8 | 45 YEARS/FEMALE | LEFT | LID SWELLING |
| 9 | 23 YEARS/MALE | RIGHT | LID SWELLING WITH CONJUNCTIVAL SWELLING |
| 10 | 33 YEARS/MALE | LEFT | PROPTOSIS WITH CONJUNCTIVL SWELLING |
| 11 | 48 YEARS/FEMALE | RIGHT | PROPTOSIS |
| 12 | 55 YEARS/FEMALE | RIGHT | PROPTOSIS |
| 13 | 37 YEARS/MALE | RIGHT | PROPTOSIS |
| 14 | 50 YEARS/FEMALE | LEFT | LID SWELLING WITH CONJUNCTIVAL SWELLING |
| 15 | 55 YEARS/FEMALE | LEFT | PROPTOSIS |
| 16 | 43 YEARS/FEMALE | LEFT | LID SWELLING |
Table 2 OUTCOMES OF INTRALESIONAL BLEOMYCIN
| S.NO | AGE/SEX | NO.OF INJECTIONS | OUTCOME AT FOLLOW-UP 1 YEAR |
|---|---|---|---|
| 1 | 5 YEARS/MALE | 2 | COMPLETE RESOLUTION |
| 2 | 10 YEARS/FEMALE | 4 | COMPLETE RESOLUTION |
| 3 | 10 YEARS/MALE | 2 | COMPLETE RESOLUTION |
| 4 | 8 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
| 5 | 5 YEARS/FEMALE | 3 | RECURRANCE AT 6 MONTH FOLLOW UP |
| 6 | 34 YEARS/MALE | 4 | COMPLETE RESOLUTION |
| 7 | 50 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
| 8 | 45 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
| 9 | 23 YEARS/MALE | 3 | NO RESOLUTION, SURGICAL EXCISION DONE |
| 10 | 33 YEARS/MALE | 3 | RECURRENCE AT 1 YEAR FOLLOW UP |
| 11 | 48 YEARS/FEMALE | 3 | NO RESOLUTION, SURGICAL EXCISION DONE |
| 12 | 55 YEARS/FEMALE | 4 | NO RESOLUTION SURGICAL EXCISION DONE |
| 13 | 37 YEARS/MALE | 4 | COMPLETE RESOLUTION |
| 14 | 50 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
| 15 | 55 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
| 16 | 43 YEARS/FEMALE | 2 | COMPLETE RESOLUTION |
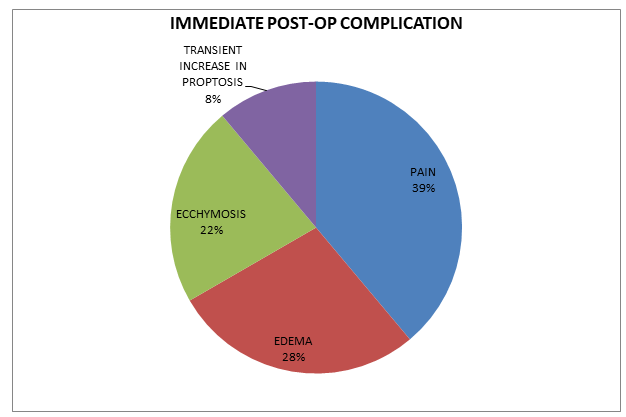
Table 3 IMMEDIATE COMPLICATION POST BLEOMYCIN

Figure 1 Ultrasound guided injection of bleomycin
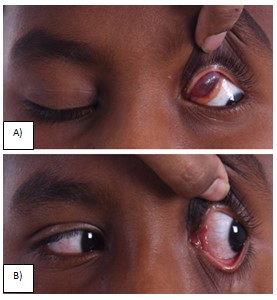
Figure 2 A ) Pre-op Left Lymphangioma B) Post bleomycin injection twice
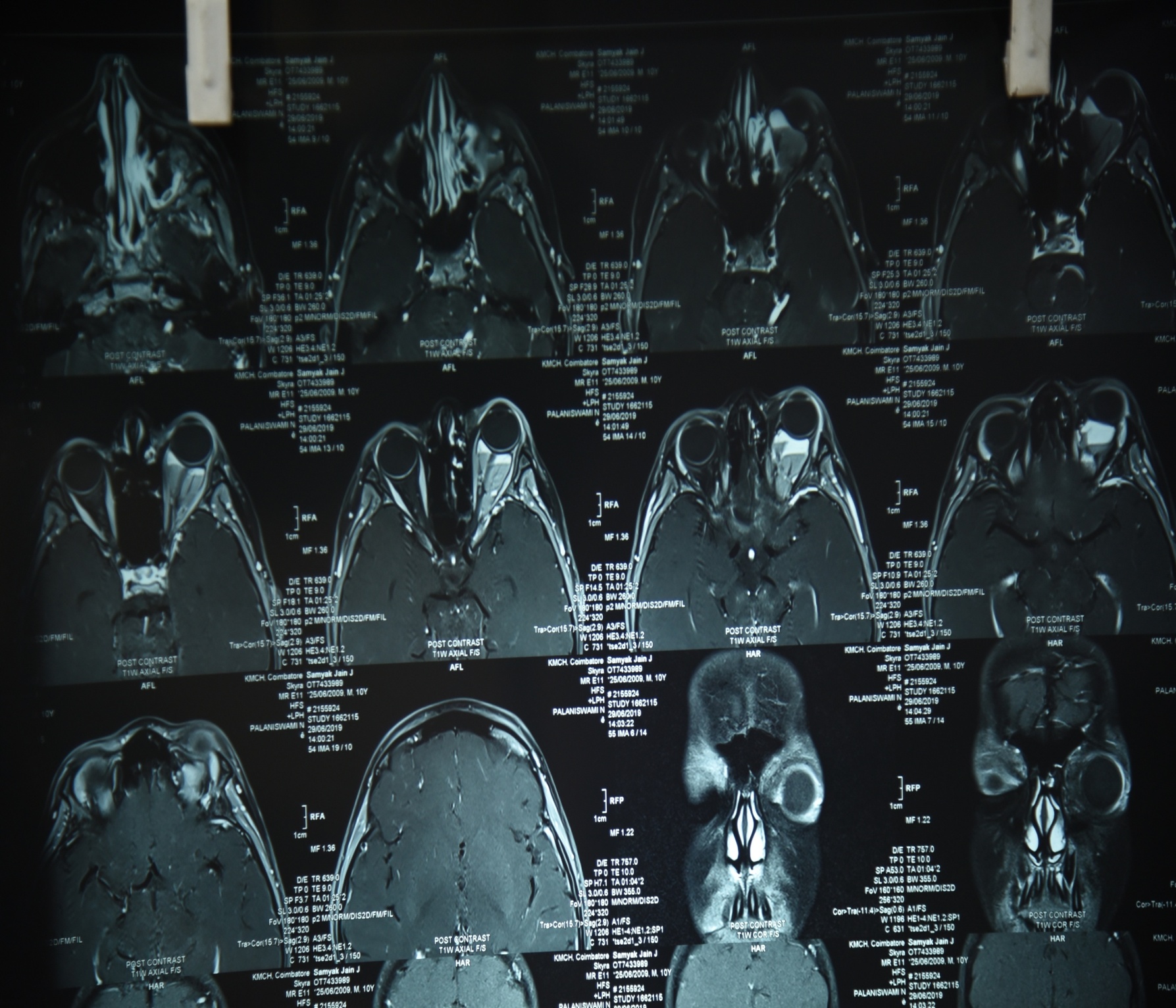
Figure 3 MRI ORBIT – PATHOGNOMIC FLUID LEVELS IN ORBITAL LYMPHANGIOMA
Leave a Comment