
 FP1637 : TRASH TO TREASURE RETCAM- TREASURE TO SAVE SIGHT AMIDST PANDEMIC
FP1637 : TRASH TO TREASURE RETCAM- TREASURE TO SAVE SIGHT AMIDST PANDEMICDr. MAHESHWARI S
DR. PRITHVI CHANDRAKANTH, Dr. RODNEY JOHN MORRIS, Dr. NARENDRAN V.
Semi Final
Abstract
To evaluate diabetic retinopathy(DR) screening at vision centres in rural and underserved areas in Tamil Nadu.
Tele-ophthalmology screening and referral for patients with Diabetic retinopathy from 11vision centres within a time span of 6months.Known and newly diagnosed diabetic patients presenting with history of reduced vision were subjected to dilated fundus evaluation with trash to treasure RETCAM by trained optometrists. Patients were diagnosed and graded DR by a remote expert. Of the 1904 patients presenting to vision centres, 851(45%)patients were diabetics. 71(8%) patients were diagnosed with DR changes of which 49(69%) patients were immediately referred to higher centre for further management. Trash to treasure RETCAM is a simple DIY smart phone based fundus imaging tool which can help in remote diagnosis of fundus pathology in an efficient way during this pandemic times eliminating unnecessary referrals.
Full Text
ABSTRACT
To evaluate diabetic retinopathy (DR) screening at vision centres in rural and underserved areas in Tamil Nadu. Teleophthalmology screening and referral for patients with Diabetic retinopathy from 11 vision centres within a time span of 6 months. Known and newly diagnosed diabetic patients presenting with history of reduced vision were subjected to dilated fundus evaluation with trash to treasure RETCAM by trained optometrists. Patients were diagnosed and graded DR by a remote expert. Of the 1904 patients presenting to vision centres, 851 (45%) patients were diabetics. 72(8%) patients were diagnosed with DR changes of which 49 (69%) patients were immediately referred to higher centre for further management. Trash to treasure RETCAM is a simple DIY smart phone based fundus imaging tool which can help in remote diagnosis of fundus pathology in an efficient way during this pandemic times eliminating unnecessary referrals.
INTRODUCTION:
Diabetes mellitus (DM) is a global epidemic. Its prevalence in India has increased from 61.3 million in 2011 to 77 million in 2019; a further 77 million are considered to be prediabetic and is projected to grow to a 101 million by 2030 and 134.2 million by 20451, 2. With over 77 of the 463 million people suffering from diabetes mellitus (DM) globally residing in India, it is said to be the diabetic capital of the world3.
Diabetic retinopathy is the most common ocular microvascular complication4. The National Survey 2015–2019 reported that 16.9% of those with DM had diabetic retinopathy (DR) in India, and 3.6% had Sight‑threatening DR (STDR).5 The progression of the disease is diagnosed through different stages ranging from Very Mild Non-Proliferative diabetic retinopathy (VMNPDR) to Moderate Non-Proliferative diabetic retinopathy (MODNPDR) stages, which are largely asymptomatic, to severe NPDR and proliferative diabetic retinopathy stages, which are potentially blinding if left untreated6. Proliferative DR and diabetic macular oedema are two main sight‐threatening components of DR (STDR)7.
According to the WHO, screening should be done for diseases that are an important health problem, have effective treatment which is possible to be delivered early, before the appearance of symptoms, technology for diagnosis is available, screening is feasible and cost effective, and subjects can be followed longitudinally. Diabetic retinopathy screening meets the World Health Organization (WHO) criteria for screening programs8.
Screening for DR is essential as individuals with DR are often asymptomatic during the earlier stages7. It is recommended that DR screening be done for all people with known diabetes on treatment, a single record of random blood sugar (RBS) of ≥ 200mg/dl (≥11.1 mmol/l), glycated haemoglobin (HbA1C) > 6.5% (48 mmmol/l) or higher or gestational diabetes when first notified to a medical personnel9. Early detection of DR by regular screening can help in slowing the progression of any DR to STDR with good control of modifiable risk factors like hyperglycaemia, hypertension, and treatment of dyslipidaemia10. Various models of DR screening applied in India are: 1) Hospital based screening model, 2) community-based screening model, 3) Teleophthalmology Screening model10.
At present situation of pandemic, Teleophthalmology plays a very important role in screening of DR patients by bridging the gap of distance, time and burden on manpower. The available devices for screening of DR can be divided into table‐top and smartphone‐based devices11.
The gold standard for grading the severity of DR is stereoscopic fundus photography through dilated pupils, using seven standard fields, and grading guidelines for these photographs established by the Early Treatment Diabetic Retinopathy Study (ETDRS) group12. Smartphone based retinal imaging system, is reasonably sensitive and specific in detecting diabetic retinopathy of varying severity and can be tried as an effective screening tool for diabetic retinopathy.10
T3 Retcam is one such Do It Yourself smartphone based imaging modality used for screening various retinal pathologies. This device was supplied to these centres which could not afford higher fundus imaging devices. Trash To Treasure Retcam remained the only option for screening.
To evaluate diabetic retinopathy (DR) screening using T3Retcam at vision centres in rural and underserved areas in Tamil Nadu for tele ophthalmology during the pandemic .
MATERIALS AND METHODS:
It is a prospective hospital-based study conducted at 11 vision centres over the time span of 6 months (January 2021 – June 2021). Study participants were known and newly diagnosed diabetic patients presenting to vision centre. Informed and written consent were obtained.
Detailed history of patients regarding name, age, sex, occupation, and address; drug history; any history of trauma or inflammation, presenting symptom, duration, and associated conditions; and medical history were recorded.
Visual acuity and refraction were assessed using an illuminated Snellen’s chart, and the ETDRS classification system was used to classify the best-corrected visual acuity.
Ocular examination was done to rule out any abnormality in the lids, conjunctiva, cornea, anterior chamber depth, iris, pupil, and lens with a torchlight.
The patients were then taken up for fundus photography by T3 Retcam which were operated by trained technicians. (Picture 1)
The images were then analysed remotely by Retinal surgeon and grading was done with Early Treatment Diabetic Retinopathy Study (ETDRS) grading system. Patients requiring intervention were then referred to tertiary hospital.
RESULTS:
Over a period of 6 months, 1904 patients visited 11 vision centres. Out of which 851 diabetics (44.69 %) were screened for Diabetic retinopathy changes. 11 patients were known diabetic retinopathy and 61 patients were newly diagnosed with diabetic retinopathy. Of the 72 patients with diabetic retinopathy, 49 patients were referred to tertiary eye hospital for further examination and management. The mean age of patients in the study group was 54.4+/-8.2 years.
Out of 49 referred patients 35 patients visited retina clinic and rest were lost to follow up. 56 eyes of 35 patients were diagnosed to have vision threatening diabetic retinopathy and was referred in need of treatment to tertiary hospital. After clinical examination and multimodal imaging at retina clinic in tertiary hospital 45 eyes i.e., 80.35% were advised treatment.
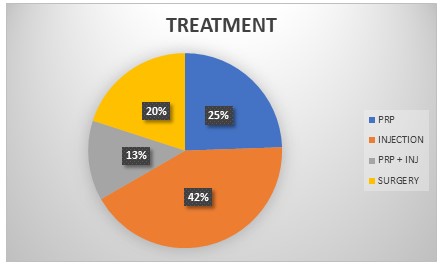
Out of 45 eyes, 11 eyes required Panretinal photocoagulation (PRP), 19 eyes required intravitreal Anti-VEGF and steroid injections, 6 eyes required intravitreal injections and PRP, 9 eyes needed surgery. (Graph 1 )
DISCUSSION:
Teleophthalmology plays an important role in screening of many diseases, DR being one of the most important ocular disease among them. Preventive care of DR focuses on screening of retinal images to evaluate the presence or absence of DR or sight‐threatening DR. It is part of routine annual diabetes preventive care. Diagnostic care involves treating or investigating sight‐threatening DR. It may include treatment for diabetic macular oedema or proliferative diabetic retinopathy (PDR), ongoing care of patients with DR, and multimodal imaging tests needed to manage or treat DR.13 Smartphone based devices play important role in preventive care of DR.
T3Retcam is one of such smart phone based device. Taking into consideration of the simplicity, stability, and affordability of the device; nevertheless, the portability, data storage capacity, and wireless connectivity of the smartphone make the T3 Retcam an important tool for screening of retinal disease.14 The T3R is shown to have a sensitivity of 88.4% and a specificity of 100% when compared with direct ophthalmoscope. The Trash To Treasure Retcam has been able to pick up larger findings/signs (Dot and Blot haemorrhage, hard exudate, soft exudate, superficial haemorrhage, IRMA, NVE, NVD, Tractional bands, Laser marks, CSME) which pose a threat to the vision. Although it is known to misdiagnose cases of VMNPDR group due to chances of missing microaneurysms 15.
Due to COVID -19 pandemic, there has been compromise in medical care, including screening programmes.16 Patient coming for routine DR check-up and screening to retina specialists has been affected in view of travel restrictions and escalating infections. In areas with effective infection control and low community transmission it is believed that DR screening can be continued safely, especially when incorporating advances in telemedicine.17
Pre-specialist diagnostics will identify healthy eyes, make a diagnosis and recommend a referral only if intervention is required. This will make the system less dependent on expensive human resources and will lead to optimal use of current resources which is of utmost importance during the pandemic.
Screening Diabetic patients at vision centres using T3Retcam associated with multi-speciality eye hospital is a very good alternative during COVID 19 outbreak.
CONCLUSION:
T3 Retcam is an inexpensive, quick, convenient, and portable device, with high sensitivity, specificity, and diagnostic accuracy for diabetic screening. It helps reduce morbidity of patients who are at a high risk of vision loss during pandemic situation.
References
1. International Diabetes Federation. IDF Diabetes Atlas. 9th ed. Brussels: Belgium; International Diabetes Federation, 2019. Available from: https://www.diabetesatlas.org/en/resources/. [Last accessed on 2021 May 17].
2. Anjana RM, Deepa M, Pradeepa R, Mahanta J, Narain K, Das HK, et al. Prevalence of diabetes and prediabetes in 15 states of India: Results from the ICMR-INDIAB population-based cross-sectional study. Lancet Diabetes Endocrinol 2017;5:585-96.
3. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International diabetes federation diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843.
4. Nentwich MM, Ulbig MW. Diabetic retinopathy ‐ ocular complications of diabetes mellitus. World J Diabetes 2015;6:489‐99.
5. Vashist P, Senjam SS, Gupta V, Manna S, Gupta N, Shamanna BR, et al. Prevalence of diabetic retinopahty in India: Results from the National Survey 2015‐19. Indian J Ophthalmol 2021;69:3087‐94.
6. Sivaprasad S, Gupta B, Crosby Nwaobi R, Evans J. Prevalence of diabetic retinopathy in various ethnic groups: Aworldwide perspective. Surv Ophthalmol 2012;57:347 70.
7. Wong TY, Sun J, Kawasaki R, Ruamviboonsuk P, Gupta N, Lansingh VC, et al. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for screening, follow‐up, referral, and treatment based on resource settings. Ophthalmology 2018;125:1608‐22.
8. Wilson JMG, Jungner G, Organization WH. Principles and Practice of Screening for Disease. Geneva: World Health Organization;1968. Available from: https://apps.who.int/iris/handle/10665/37650.[Last accessed on 2021 May 17].
9. Raman, Rajiv; Ramasamy, Kim1; Rajalakshmi, Ramachandran2; Sivaprasad, Sobha3; Natarajan, S4 Diabetic retinopathy screening guidelines in India, Indian Journal of Ophthalmology: March 2021 – Volume 69 – Issue 3 – p 678-688 doi: 10.4103/ijo.IJO_667_20
10. Rajalakshmi R, Prathiba V, Mohan V. Does tight control of systemic factors help in the management of diabetic retinopathy?. Indian J Ophthalmol 2016;64:62‐8.
11. Ramasamy K, Mishra C, Kannan NB, Namperumalsamy P, Sen S. Telemedicine in diabetic retinopathy screening in India. Indian J Ophthalmol. 2021 Nov;69(11):2977-2986. doi: 10.4103/ijo.IJO_1442_21. PMID: 34708732; PMCID: PMC8725153.
12. American Diabetes Association. . Diabetic retinopathy Diabetes Care. 2000;23(Suppl 1):S73–6
13. Raman R, Dasgupta D, Ramasamy K, George R, Mohan V, Ting D. Using artificial intelligence for diabetic retinopathy screening: Policy implications. Indian J Ophthalmol 2021;69:2993-8.
14. Chandrakanth, Prithvi; Ravichandran, Ramya; Nischal, Naveen G; Subhashini, M Trash to treasure Retcam, Indian Journal of Ophthalmology: April 2019 – Volume 67 – Issue 4 – p 541-544 doi: 10.4103/ijo.IJO_1524_18
15. Chandrakanth P, Chandrakanth KS, Vishwanathan AS, Nirupama R, Mathew T. Efficacy of trash to treasure retcam in diabetic retinopathy screening. Kerala Journal of Ophthalmology. 2020 Sep 1;32(3):278.
16. Abbasi K. The scandals of covid-19. Editorial. BMJ. 2020;369:m1434. doi: 10.1136/bmj.m1434.
17. Shih KC, Kwong AS, Wang JH, Wong JK, Ko WW, Lai JS, Chan JC. Diabetic retinopathy screening during the coronavirus disease 2019 pandemic. Eye. 2020 Jul;34(7):1246-7.
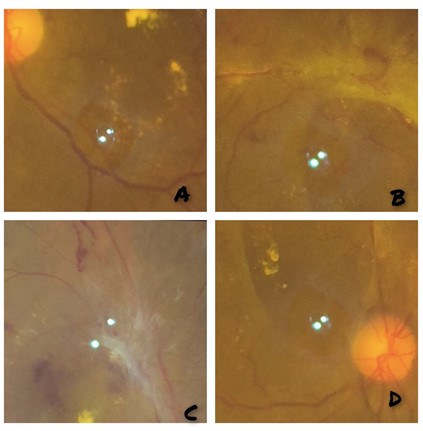
PICTURE 1: A: Hard exudates at macula suggestive of Clinically significant macular oedema, B and C: Fibrous proliferation with Neovascularisation at arcades suggestive of Proliferative Diabetic Retinopathy, D: Early fibrous proliferation at disc suggestive of Proliferative diabetic retinopathy.
Leave a Comment