
 FP0440 : ACUTE ACQUIRED COMITANT ESOTROPIA PRECIPITATED BY EXCESS NEAR WORK DURING COVID-19 HOME CONFINEMENT
FP0440 : ACUTE ACQUIRED COMITANT ESOTROPIA PRECIPITATED BY EXCESS NEAR WORK DURING COVID-19 HOME CONFINEMENTDr.Neena.R
Abstract
To evaluate the causes of AACE in young adults and children during the COVID-19 induced home confinement.A retrospective,clinical study of all,who presented to a tertiary eye care center in South India,during the COVID-19 pandemic(August 2020-January 2021)with acute-onset,non accommodative comitant esotropia.Majority;11(73.3%)} of the total 15 patients were students>10 years(mean age=16.8 years).Most;12(80%) had >8 hours of near activity/day with(mean= 8.6 hours/day).The most common near activity was online classes,followed by job related work and mobile games.86.7% used smart phones for near work.The average esotropia was 22.73 PD for distance and 18.73 PD for near.Majority (66.6%),had low-moderate hyperopia with basic or divergence insufficiency esotropia and the remaining 33.3% with myopia fitted in to the Bielschowsky type AACE.The habit of long-time sustained near work,especially on smart phones may increase the risk of inducement of AACE
Full Text
ABSTRACT
To evaluate the causes of AACE in young adults and children during the COVID-19 induced home confinement. A retrospective, clinical study of all, who presented to a tertiary eye care center in South India during the COVID-19 pandemic (August 2020-January 2021)with acute-onset, non accommodative comitant esotropia. Majority;11(73.3%)} of the total 15 patients were students>10 years(mean age=16.8 years).Most;12(80%) had >8 hours of near activity/day with(mean= 8.6 hours/day).The most common near activity was online classes, followed by job related work and mobile games.86.7% used smart phones for near work.
The average esotropia was 22.73 PD for distance and 18.73 PD for near. Majority (66.6%) had low-moderate hyperopia with basic or divergence insufficiency esotropia and the remaining 33.3% with myopia fitted in to the Bielschowsky type AACE. The habit of long-time sustained near work, especially on smart phones may increase the risk of inducement of AACE
INTRODUCTION:
The COVID-19 pandemic, caused by the novel coronavirus SARS-CoV2 has changed life dramatically for us; both at work and at home. Global number of workers working from home is now estimated at 558 million, corresponding to 17.4% of global employment (Berg et al. 2020, ILO 2020). Schools and colleges across the country started to shut down temporarily by the second week of March 2020, to contain the spread of the novel coronavirus1.
Around 320 million learners have transitioned to e-learning since then. The increasing use of gadgets for studies, work and leisure prompted by the pandemic has led to cropping up of many health problems in the students including weight gain, sleep disruption, and psychosocial stress2.The worsening dependence on digital devices during the COVID-19 pandemic and its negative impact on student’s eye health including that of computer vision syndrome and increased risk of myopia has raised some serious concerns3.
Ever since the country wide lockdown due to Covid-19 began and with the new norm of “work, study and play from home”, we saw a substantial number of children and young adults with complaints of recent onset of squinting and diplopia coming to the Pediatric ophthalmology & Strabismus services of our hospital. This prompted us to devise this study.
Acquired non-accommodative esotropia (ANAET) is a relatively rare, distinct subtype of esotropia characterized by a non-accommodative esodeviation which can occur in older children, adults, and even the elderly4,5 It can result from deterioration of existing, previously controlled, esophoria or can present acutely with diplopia when it is called acute acquired comitant esotropia (AACE) 6,7 AACE contributes to about 0.3% of childhood strabismus. AACE can be divided into five different subtypes8-12. The Swan type (Type I) occurs after a period of interrupted binocularity9.
Type II AACE, known as Burian-Franceschetti, has minimal hypermetropia and diplopia that are often associated with physical or psychological stress10. The Bielschowsky type (Type III) is associated with patients with myopia, convergence spasm, and divergence paralysis11.Type IV/refractive-accommodative type is characterized by high hypermetropia that can be adequately controlled with the refractive correction alone12. Type V, a lesser common entity, is associated with intracranial pathology, most commonly a posterior fossa lesion13. In a small retrospective noncomparative study of 10 adult patients with acute-onset concomitant esotropia, Spierer14 found that almost all were myopic, all regained normal stereopsis after surgery and suggested that they be classified as a distinct subgroup of acute-onset esotropia.
PURPOSE
To examine the causes of acute acquired comitant esotropia (AACE) in young adults and children in the setting of COVID-19 induced home confinement.
MATERIALS & METHODS
This was a retrospective, clinical study of all patients, who presented to the Pediatric Ophthalmology and Strabismus Services of a tertiary eye care center in South India, from August 2020 to January 2021 during the COVID-19 pandemic, with acute-onset, comitant esotropia.
The diagnosis of AACE was made on the following criteria:
- Acute onset of esotropia within hours/days/weeks, with photographic evidence of previously aligned eyes.
- Age of onset after 1 year of age.
- Comitant esodeviation with normal ocular movements.
Apart from the demographic parameters like age, sex, occupation/class of study, visual acuity for distance & near, binocular status for distance & near, amount and type of deviation were studied. A careful history including duration of presenting complaint, any precipitating event, previous use of glasses, nature, duration and medium of near work were taken. All patients underwent a meticulous ocular examination including a dilated fundus examination. Cycloplegic refraction was done with atropine in all to detect true refractive status and to rule out accommodative esotropia. A detailed orthoptic evaluation was also performed. Occlusion therapy was started in all children detected to have amblyopia or at risk of amblyopia. All patients underwent magnetic resonance imaging (MRI) of the brain and orbits to rule out intracranial pathology as well as a neurology evaluation. The minimum follow-up period was 6 months. The study was conducted in accordance with the Declaration of Helsinki, and was approved by the appropriate Institutional Review Board and Ethics committee.
We found 4 categories of patients with AACE in our study:
- Those with myopia (SE>=-0.5DS) and divergence insufficiency (distance esotropia > near esotropia) and occasionally equal deviation for distance and near as described by Bielschowsky11.
- Those with low hyperopia (SE<=2DS) and divergence insufficiency esotropia
- Those with low hyperopia (SE<=2DS) and basic type esotropia (difference between distance and near esotropia not >5PD)
- Those with moderate hyperopia (SE=2.25-5DS), with esotropia precipitated by stress (fever prior to onset of esotropia in our patient).
The only common factor in all these patients with esotropia was excessive near work either on smart phone, laptop or books except in one patient with low hyperopia and divergence insufficiency esotropia who denied any over use of near work.
RESULTS
We had total 15 cases of acute esotropia in our study; 11 males and 4 females. The age ranged from 5 years to 24 years with majority above 10 years and with a mean age of 16.8 years (SD: 5.659). Majority; 11 (73.3%)} were students and the rest 4(26.7%) were employed. Most patients (73.3%) presented with diplopia and squint, whereas 6 (40.0%) had diplopia alone and 2 (13.3%) presented with squint alone. The mean duration of presentation was 2.98months (SD: 4.790) and ranged from 15 days to 6 months. There was no precipitating event other than excess near work in the majority except in one patient who had fever prior to the onset of esotropia. MRI of the Brain was done in all and were unremarkable, Duration of near work ranged from 3-12 hours a day with a mean duration of 8.6 hours/day. Most; 12(80%) had more than 8 hours of near activity. The near activity was related to online classes in 8 (53.3%), official work in 3(20%), mobile games in 3(20%) and religious text reading in 1(6.7%) respectively.
The medium of near work was mainly smart phone alone in 13 patients (86.7%), smart phone and laptop in 1 patient(6.7%) and books in 1 patient (6.7%).Most; 9(60%) in our study had low hyperopia (SE<=2DS), 1(6.6%) had moderate hyperopia (2.25-5DS SE) and the remaining 5(33.3%) had myopia (SE>=-0.5DS). Seven patients (46.7%) were using glasses at the time of presentation, of which 5 (33.3%) had myopia. Three (60.0%) out of the five with myopia admitted to doing near work without glasses. Eleven patients (73.3%) had diplopia, 1 had fusion and the rest 3 were suppressed on Worth Four Dot Test (WFDT) for distance. The mean stereopsis for near was 116.67 and ranged from 40-400 arc seconds using the Randot® Stereotest.. The average esotropia for distance was 22.73 Prism Diopter(PD) and ranged from 10-40 PD; whereas for near it was 18.73 PD and ranged from 2 -45 PD. Orthoptic evaluation revealed average Near Point of Accommodation(NPA) of 6 (SD=1.664), average Near Point of Convergence (NPC)of 5.36(SD=1.689),average Negative Relative Accommodation(NRA) of 3.33 (SD=1.033), average Monocular Estimation Method(MEM) of 0.76(SD= 0.305)and an average Accommodative Convergence/Accommodation(AC/A) ratio of 5.40 (SD=3.638).There was high Positive Relative Accommodation(PRA>-3.5)in 8(53.3%) and the rest had normal (PRA<=3.5)values. Reduced or poor Negative Fusional Vergence (NFV) for distance was seen in 40% patients.
On accommodative facility testing; 26.66% complained of difficulty in clearing plus lenses, 13.33% had difficulty clearing minus lenses, 46.66% had reduced binocular accommodative facility and only 2(13.33%) had normal facility. Most of those with myopia (3 out of 5) had high AC/A ratio, accommodative lag(4 out of 5) on MEM but had esodeviation more for distance than near contrary to the expectation. All 5(33.33%) of those with myopia fitted in to the Bielschowsky type of AACE with 4 of them having divergence insufficiency and the remaining 1 having basic type AACE. One patient with moderate hypermetropia and diplopia, had fever preceding the onset of esotropia, was prescribed plus lenses and could be classified as Burian-Franceschetti type of AACE. The remaining 9(60%) had low hyperopia with either basic type AACE (33.3%) or divergence insufficiency type AACE (26.7%). All were advised to restrict and reduce their near work, those with glasses were advised constant use and those with divergence insufficiency were prescribed divergence exercises or prisms. Reduction of near work with divergence exercises was helpful in 5 patients in our study Those with basic type AACE, who did not improve were advised squint surgery. Ground prisms in glasses were prescribed for 2 patients, both with myopia and divergence insufficiency type AACE(3 PD BO OU & 6 PD BO OD respectively). Four patients; 3 with low hyperopia and basic type AACE and 1 with Burian-Franceschetti type of AACE underwent squint surgery and regained binocular vision (Figures 1 a, b, 2a, b.3a, b,4a,b) and Tables 1 & 2.
DISCUSSION
Continuing school closure, home confinement and work from home policies during the current COVID-19 lockdown have ushered in important lifestyle behavior changes in the young population, including a significant increase in screen time15, digital eye strain and raised serious concerns of worsening the global burden of myopia3.Apart from these, the excessive application of near vision might have other undesirable effects, including development of acute acquired concomitant esotropia.. Lee et al16documented a series of 12 teenagers with acute acquired concomitant esotropia who used smartphones more than 4 hours a day. Interestingly, the esodeviation improved in all patients after refraining from smartphone use for 1 month.
Nevertheless, strabismus surgery was required in 5 patients with good postoperative outcomes in terms of ocular alignment and stereo acuity. The average duration of smartphone use in their study was 6.08 ± 1.78h/day, which was similar to 8.6h/day of near work in our study. In a retrospective study of 26 cases with AACE over 20 months; Yan Wu etal17 deduced that AACE could be caused by excessive near work regardless of whether or not one wears glasses regularly especially for individuals with myopic refractive error. The only common factor that contributed to the development of AACE in their study was also the excessive near visual activities, especially the use of smartphones.
In our study, majority (66.6%), had low hyperopia with basic or divergence insufficiency esotropia and the remaining 33.3% had myopia which fitted in to Bielschowsky type AACE.. Excessive near work and a naturally stronger convergence in the young could have led to an imbalance between accommodation and vergences resulting in dynamic activation of the medial rectus muscles and a manifest esodeviation. This effect is greater in hyeropes due to their greater accomodative demand as also seen in our study with 66.7% having hypermetropia. Conventionally, it is thought that the presence of myopia is associated with a decreased demand for accommodation and hence lower convergence and a predisposition for developing exotropia.
However, those with myopia, can also develop esotropia due to the excessive application of near work resulting in increased tone of medial rectus muscles and coupled with the lack of distant stimuli during the home confinement leading to divergence weakness was also seen in our study. Bielschowsky11claimed that uncorrected myopia led to the development of increased tonus of the medial rectus muscles and suggested that the increase in tonus can be explained by the tendency of individuals with uncorrected myopia to hold print or sewing excessively close to the eyes, with resulting development of esotropia. 60% of those with myopia in our study also admitted to doing near work without glasses as they felt they could see clearly. In a well-defined study of adult patients with acute-onset concomitant esotropia by Sprier etal14, almost all were myopic, and all regained normal stereopsis after surgery.
In a retrospective, clinical study of all patients under the age of 18 years with acute onset, non-accommodative comitant esotropia, we18 had earlier reported that prompt amblyopia therapy and timely surgery can result in a satisfactory outcome in those without systemic involvement. In our present study also, reduction of near work with divergence exercises was helpful in 5 patients. Two patients were given prism glasses, 4 underwent squint surgery, 3 were advised glasses and squint correction and 1 was awaiting squint surgery. All who underwent squint surgery regained binocularity and were diplopia free. Aldo Vagge etal19described four cases of acute acquired concom¬itant esotropia that occurred during the COVID-19 lockdown in Italy in 2020, wherein all patients spent 8 to 10 hours a day using computers, tablets, and smartphones to play, access school lessons, and navigate social networks. In a similar case setting of COVID-19 induced home confinement, we are reporting a case series of 15 patients with AACE.
Although the etiology of acute acquired concomitant esotropia is still debated, it has been associated with sustained near point demands due to the excessive use of computers, tablets, and smartphones. With the increasing use of smartphones and tablets in modern life, more and more work is being done through small screens at a close distance. We feel that this excessive near work, a naturally stronger convergence and lack of distance stimuli could have led to an imbalance between accommodation and vergences, resulting in dynamic activation of the medial rectus muscles with or without divergence weakness, thus producing a manifest esotropia in our patients.
We feel that sustained near work played a pivotal role in the development of esotropia in our patients and hope that authorities would take serious note of this this undesirable effect. Regulating the duration of e- learning, reducing the number of total hours of screen time, shifting to widescreen visual display devices like television, taking breaks, promoting healthy life style habits like increasing outdoor play should be recommended to improve the eye health of the young population.
CONCLUSION:
The habit of long-time sustained near work, especially on smart phones may increase the risk of inducement of AACE. Parents and public health authorities should take serious note of this negative impact on the eye health of the young population and should bring out suitable recommendations and regulations to mitigate this undesirable effect.
REFERENCES
- Available from: https://government.economictimes.indiatimes.com/news/education/covid-19-pandemic-impact-and-strategies-foreducation-sector-in-india/75173099
- Wang G, Zhang Y, Zhao J, Zhang J, Jiang F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet. 2020; 395(10228):945-947. Doi: 10.1016/S0140-6736(20)30547-X
- Pellegrini M, Bernabei F, Scorcia V, Giannaccare G. May home confinement during the COVID-19 outbreak worsen the global burden of myopia? Graefes Arch Clin Exp Ophthalmol.2020; 258(9):2069-2070. Doi: 10.1007/s00417-020-04728-2
- Legmann Simon A, Borchert M. Etiology and prognosis of acute, late onset esotropia. Ophthalmology 1997; 104:1348 52.
- ClarkAC, Nelson LB, Simon JW, Wagner R, Rubin SE. Acute Acquired Comitant Esotropia. Br J Ophthalmol1989; 73:636 8.
- Lyons CJ, Tiffin PA, Oystreck D. Acute Acquired Comitant Esotropia: A prospective study. Eye (Lond) 1999; 13 (Pt 5):617 20.
- Sturm V, Menke MN, Töteberg M, Jaggi GP, Schoeffler C. Early onset of acquired comitant non accommodative esotropia in childhood. KlinMonblAugenheilkd2012; 229:357 61.
- Burian HM, MillerJE. Comitant convergent strabismus with acute onset. Am J Ophthalmol1958; 45:55 64.
- Swan KC. Esotropia following occlusion. Arch Ophthal1947; 37:444 51.
- Franceschetti A. Acute concomitant strabismus. Ophthalmologica1952; 123:219 26.
- Bielschowsky A. Das einwärtsschielen der myopen [Convergent strabismus of myopes]. Ber DtschOphthalmolGes1922; 43:245-59.
- VonNoorden GK. Esodeviations. In: von Noorden GK, Campos E, editors. Theory and Management of Strabismus in Binocular Vision and Ocular Motility. 5th ed. USA: The C.V. Mosby Company; 1990. p. 309.
- Astle WF, Miller SJ. Acute comitant esotropia: A sign of intracranial disease. Can J Ophthalmol1994; 29:151 4.
- Spierer A. Acute concomitant esotropia of adulthood. Ophthalmology. 2003; 110:1053–6.
- Bahkir FA, Grandee SS. Impact of the COVID-19 lockdown on digital device-related ocular health. Indian J Ophthalmol. 2020; 68:2378–83.
- Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive Smartphone use. BMC Ophthalmol. 2016; 16(1):37. Doi: 10.1186/s12886-016-0213-5
- Yan Wu, Shuan Dai, Xue Liang Feng and Bin Sun. (2020). Excessive Smartphone Use May Cause Acute Acquired Comitant Esotropia. Journal of Ophthalmology and Vision Research 2(1).
- Neena R, Giridhar A. Acute acquired comitant esotropia in children: A benign entity or an ominous sign? Kerala J Ophthalmol 2019; 31:33-8.
- Aldo Vagge, MD, PhD; Giuseppe Giannaccare, MD, PhD; Fabio Scarinci, MD, PhD; Andrea Cacciamani, MD; Marco Pellegrini, MD; Federico Bernabei, MD; Vincenzo Scorcia, MD; Carlo E. Traverso, MD; Donatella Bruzzichessi, MD.Acute Acquired Concomitant Esotropia From Excessive Application of Near Vision During the COVID-19Lockdown.J PediatrOphthalmolStrabismus. 2020; 57:e88-e91.
APPENDIX: FIGURES
Figure: 1(a) -Patient A at 1.5 years. Figure:1(b) -Patient A ( PUBG addict) before & after surgery

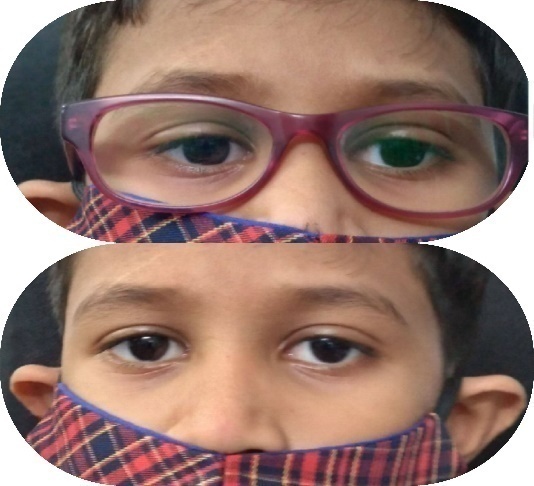
Figure:2(a) -Patient B 6 months before with straight eyes: 2(b) – Patient B (Class X student with 8 hours/day of online classes on smart phone); with basic type esotropia Left eye before and straight eyes after surgery


Figures:3(a) -Patient C (using smartphone for online classes and games > 8 hours/day); showing basic type esotropia Right eye, 3(b) -Patient C showing straight eyes post Right eye surgery (Medial Rectus recession+ Lateral Rectus resection).


Figure: 4(a) Patient D before :17 year old, college student who developed AACE with >8 hours of near work on smart phone ; Figure: 4(b) Patient D after surgery(Medial Rectus Recession +Lateral Rectus Resection)


TABLE:1 CLINICAL PROFILE OF PATIENTS WITH AACE
| SL NO | Age(Years) | Sex | Presenting complaints | Wearing spectacles | Hours of near work/day | Type of near work |
|---|---|---|---|---|---|---|
| 1 | 24 | M | Diplopia | YES | 6 | job related |
| 2 | 17 | M | Diplopia & Squint | NO | 8 | Religious text reading |
| 3 | 8 | M | Squint | NO | 8 | mobile games, you tube |
| 4 | 15 | F | Diplopia & Squint | YES | > 8 | online classes |
| 5 | 15 | M | Diplopia | NO | 6 | online classes |
| 6 | 20 | M | Diplopia | NO | >8 | online classes |
| 7 | 16 | M | Diplopia | NO | > 8 | online classes |
| 8 | 20 | M | Diplopia & Squint | YES | 12 | mobile games, you tube |
| 9 | 24 | M | Diplopia | YES | >8 | job related |
| 10 | 5 | M | Squint | NO | >10 | PUBG game |
| 11 | 16 | F | Diplopia | YES | 12 | online classes |
| 12 | 20 | F | Diplopia & Squint | NO | >12 | Online classes, SOCIAL MEDIA |
| 13 | 23 | M | Diplopia & Squint | YES | >12 | job related |
| 14 | 19 | F | Diolopia and Squint | NO | 3 | Online classes |
| 15 | 10 | M | Diplopia & Squint | YES | 8 | Online classes |
TABLE 2 : FEATURES OF ESOTROPIA
| ESOTROPIA(Distance) BO | ESOTROPIAT(Near)BO | TYPE OF ET | WFDT for Distance | Stereopsis for Near | REFRACTIVE ERROR | IMPRESSION FROM ORTHOPTIC EVALUATION | MRI BRAIN & ORBITS | IMPROVEMENT WITH REDUCTION OF NEAR WORK | OTHER TREATMENT GIVEN |
|---|---|---|---|---|---|---|---|---|---|
| 12 BO | 5BO | ET D>N | DIPLOPIA | 60 | MYOPIA | HIGH AC/A, ACCOMODATIVE LAG, REDUCED FUSIONAL DIVERGENCE, ET D>N | normal | YES | 3 PRISM BO OU |
| 40 BO | 45 BO | BASIC | DIPLOPIA | 140 | LOW HYPEROPIA | NORMAL AC/A, NORMAL MEM, HIGH PRA, BASIC ET | normal | NO | OO (MR recession 6mm+ LR resection 8mm)under LA |
| 30 BO | 30BO | BASIC | RIGHT SUPPRESSION | 400 | LOW HYPEROPIA | HIGH AC/A, ACCOMODATIVE LAG, BASIC ET | normal | NO | (OD MR recession 5mm+LR resection 5mm) |
| 35 BO | 30BO | BASIC | DIPLOPIA | CANNOT COMPREHEND | LOW HYPEROPIA | HIGH AC/A, NORMAL MEM, HIGH PRA, BASIC ET | normal | NO | (OS MR Recession 6mm+ LR resection 7.5mm) |
| 16 BO | 9 BO | ET D>N | ALT SUPPRESSION | 40 | LOW HYPEROPIA | NORMAL AC/A, HIGH NRA, NORMAL MEM , REDUCED FUSIONAL DIVERGENCE, ET D>N | normal | NO | Divergence exercises |
| 10BO | 2 BO | ET D>N | DIPLOPIA | 60 | LOW HYPEROPIA | LOW AC/A, HIGH PRA, ACCOMODATIVE LAG LAG, REDUCED FDV FOR D, ET(D>N) | normal | NO | Glasses + Divergence exercise |
| 30 BO | 30 BO | BASIC | DIPLOPIA | 140 | LOW HYPEROPIA | LOW AC/A,LOW NRA, ACCOMODATIVE LAG,BASIC ET | NO | GLASSES+ DIVERGENCE Exercises, advised Squint surgery | |
| 25 BO | 30 BO | BASIC | DIPLOPIA | 100 | MYOPIA | HIGH AC/A, HIGH PRA, ACCOMODATIVE LAG,BASIC ET | normal | NO | Glasses, advised Squint surgery |
| 12BO | 2 BO | ET D>N | DIPLOPIA. | MYOPIA | NORMAL AC/A, HIGH NRA, HIGH PRA, ACCOMODATIVE LAG REDUCED FDV ,ET(D>N) | normal | YES | 6 PRISM BO OD | |
| 35BO | 40BO | BASIC | ALT SUPPRESSION | CANOT COMPREHEND | MODERATE HYPEROPIA | HIGH AC/A,HIGH NRA,HIGH PRA,ACCOMODATIVE LAG,BASIC ET | normal | NO | (OU MR Recession 6mm) |
| 10 BO | 5 BO | ET D>N | DIPLOPIA | 100 | MYOPIA | NORMAL AC/A,HIGH NRA,LOW PRA,MEM NORMAL,REDUCED FDV ,ET(D>N) | Normal | YES | Glasses + Divergence exercise |
| 25 BO | 14 BO | ET D>N | DIPLOPIA | 100 | LOW HYPEROPIA | LOW AC/A, HIGH NRA, NORMAL MEM ,ET (D>N) | normal | NO | Glasses +Divergence exercises. |
| 16 BO | 6 BO | ET D>N | FUSION | 60 | MYOPIA | HIGH AC/A, HIGH NRA, ACCOMODATIVE LAG, ET(D>N) | Normal | YES | Glasses +Divergence exercises |
| 20 BO | 8 BO | ET D>N | DIPLOPIA | 100 | LOW HYPEROPIA | LOW AC/A, HIGH NRA,HIGH PRA.ACCOMODATIVE LAG,ET (D>N) | normal | NO | Glasses + Divergence exercise |
| 25 BO | 25 BO | BASIC | DIPLOPIA | 100 | LOW HYPEROPIA | NORMAL AC/A, NORMAL MEM, BASIC ET | normal | NO | Squint surgery advised |
Abbreviations used:
ET: ESOTROPIA
AC/A: ACCOMMODATIVE CONVERGENCE/ACCOMMODATION
MEM: MONICULAR ESTIMATION METHOD
PRA: POSITIVE RELATIVE ACCOMODATION
NRA: NEGATIVE RELATIVE ACCOMMODATION